
Abstract
Background: Hearing impairment represents a significant global health issue, affecting more than 400 million people worldwide, with projections exceeding 1 billion by 2030. Accurate audiological diagnosis is essential for early rehabilitation and improved social integration of individuals with hearing loss. While speech audiometry is commonly used to evaluate speech intelligibility, it may be difficult to perform in certain populations such as children and elderly individuals due to technical limitations, lack of equipment, and long testing times.
Objective: This study aimed to improve the effectiveness of audiological diagnostics by proposing a simpler and faster method to predict the maximum speech intelligibility score based on tonal audiometry parameters.
Methods: The study included 70 adult patients with bilateral sensorineural hearing loss and acontrol group of 18 adults with normal hearing (aged 18–59 years). Clinical evaluation included ENT examination, phonic acumetry, pure tone audiometry (PTA), and speech audiometry (SA). Air conduction thresholds were measured between 125–8000 Hz and bone conduction thresholds between 250–6000 Hz. Speech audiometry was performed by presenting speech stimuli at 20–30 dB above the hearing threshold, with 5 dB increments. Statistical analysis included regression analysis, discriminant analysis, Student’s t-test, and Fisher’s test to determine the relationship between tonal audiometry parameters and maximal speech intelligibility scores.
Results: The findings demonstrated significant correlations between pure tone audiometry parameters and speech intelligibility scores. Changes in hearing thresholds across frequencies were observed in all degrees of hearing loss, with statistically significant differences (p < 0.001). Regression analysis enabled the development of a predictive formula for estimating maximal speech intelligibility scores based on tonal audiometry results.
Conclusion: The proposed method allows prediction of maximal speech intelligibility without performing speech audiometry, reducing examination time and eliminating the need for additional equipment. This approach may facilitate faster diagnosis and rehabilitation planning for patients with hearing impairment, particularly in settings where speech audiometry is difficult to perform.
Introduction
The efficient diagnosis of deafness presents an important physical-clinical and technical problem, since adequate rehabilitation leads to the involvement of patients suffering from hearing impairment in social activity. In some cases, speech audiometry presents difficulties in performing, primarily in children and the elderly, due to the lack of specialized audiometers, calibration equipment, dialect-specific vocal audiometry tests, and the long investigation time. The proposed method allows specific diagnosis tests without vocal audiometry, not require additional devices, takes less time which is important to initiate faster medication and rehabilitation program for the hearing impaired. The advantage is in objectifying the prediction of the maximum speech intelligibility score.
Currently, there are over 400 million people in the world who suffer from deafness and this number is growing. According to estimates, in 2030, the number of people with hearing disabilities may exceed 1 billion. Hearing impairment (especially severe and profound forms) leads to a change in the position of the individual in society, to loss of working capacity, and in the case of deafness that appeared in early childhood – to deaf-muteness, mental retardation [1].
The state of residual hearing in deafness people is characterized by the following clinical and audiological indices: the results of the ENT examination, etiology, clinical diagnosis, the nature of the hearing impairment, especially the degree of hearing loss in the right and left ear, the configuration of the audiometric curve, the ratio between the tonal hearing threshold and air conduction at the frequencies of the speech area, the threshold of auditory discomfort, the dynamic range of hearing, the presence or absence of tinnitus [2,3].
The efficient diagnosis of deafness presents an important physical-clinical and technical problem, since adequate rehabilitation leads to the involvement of patients suffering from hearing impairment in social activity [4,5]. Therefore, establishing the differential diagnosis of the forms of sensorineural deafness is a crucial moment in the audiological study.
Pure tone audiometry (PTA) is the most accurate method of determining hearing thresholds based on the frequency spectrum. However, it has limitations: premature infants and adults who are unconscious or mentally ill. Although PTA is the oldest audiometric test performed with electronic equipment, it remains the most important and accurate method of determining hearing impairment and the type of hearing loss [6,7].
Speech audiometry (SA) is a method of measuring the patient's ability to understand words, i.e. what percentage of speech elements are correctly recognized at a given intensity. SA is a method of metrological study of hearing, which uses a certain phonetic material (verbal or vocal) for its tests, and examines hearing in a global manner [8,9]. PTA provides information about the sensitivity of hearing, but in terms of the interpersonal communication capacity that SA provides – only limited information. SA does not provide information about hearing sensitivity as a function of intensity-frequency. However, thresholds obtained by transmitting vocal stimulus via air provide information about hearing sensitivity as a whole, and those obtained by bone conduction – information about the neurosensory status. There are studies that predict SA indices (intelligibility score) based on PTA parameters [3, 4, 6].
In some cases, SA presents difficulties in performing, primarily in children and the elderly, due to the lack of specialized audiometers, calibration equipment, dialect-specific vocal audiometry tests, and the long investigation time [10,11]. At the same time, in order to establish the topographic diagnosis of auditory pathologies and the appropriate individual selection of hearing aids, it is important to establish the maximum intelligibility score of vocal tests. Thus, it becomes appropriate to use new principles for determining the respective index [12,13,14].
The aim of the study:
Increase the effectiveness of audiological diagnostics, thanks to a more operative and simple method of prognosis of the maximum speech intelligibility score.
Material and methods
The investigations were carried out on a group of 70 patients, adults with bilateral sensorineural deafness, control group with normal hearing – 18 adults (18-59 age). Primary clinical examination (including ENT status), phonic acumetry, pure tone audiometry, and speech audiometry were used. The method proposes to predict this index based on anamnesis data and pure tone audiometry (it is easier to perform). The material of this study included the analysis of anamnesis, clinical, instrumental data, the informativeness of various audiometric investigation methods and the selection of hearing aids.
PTA was performed by determining air conduction at 125-8000 Hz (herz) and bone conduction at 250-6000 Hz [7, 15]. SA began with the presentation of intensity of 20-30 dB (decibel) above the auditory threshold. The intensity changed in increments of 5 dB. The main components of the curve representing the maximum word recognition score were studied: undifferentiated voice threshold 20%, 50%, 80%, 100% [6,7,16]. To determine the paradoxical drop in the maximum recognition score, the investigation was performed at 100 dB intensity. The investigation was performed separately for right ear (AD) and left ear (AS).
The maximum voice intelligibility score was determined both by performing the voice audiometry [2,7,17] described above (the average time for performing voice audiometry was 25-30 min), and by evaluating the following indices of tonal audiometry: the aspect of the PTA audiometric curve (AC), the average hearing threshold (AH) established in PTA, the average level of deafness (LD) established in PTA, the average discomfort threshold (DT) established in suprathreshold PTA, the articulation index (IA) calculated based on PTA results [8].
The statistical processing of quantitative values was preceded by the calculation of the arithmetic mean (M) and the arithmetic mean error (m). The comparison of variables in different groups was carried out according to the Student criterion. The discriminant analysis method, being an integral part of the theory of mathematical methods of image identification, allows, through retrospective analysis, the establishment of prognostic regularities. Discriminant analysis consists in constructing the linear function (Fj) of the vector X [6,8].
The method was deduced allowed determining the maximum intelligibility score parameter in dB following the results of the threshold and suprathreshold pure tone audiometry. The use of regression analysis in the processing of statistical data on the investigated patients allowed us to deduce the formula proposed below, which is the essence of the diagnostic method. Deriving the regression equation from the data tonal audiometry (PTA) was performed [8]. Continuous variables were expressed as mean ± SD (standard deviation) and for the comparison between groups of continuous variables the t-student and Fisher tests were applied. The differences between the statistically significant mean values (p<0.05) and their 95% confidence interval were calculated. The calculation of the Odds Ratio (OR) and the 95% confidence interval (CI) was used to evaluate the ability of the parameters to group subjects into groups with normal or pathological values. The p value ≤ 0.05 was considered as a criterion of statistical significance, and 0.05-0.1 was considered a statistical trend.
Favorable opinions of the Research Ethics Committee of the Nicolae Testemițanu State University of Medicine and Pharmacy No. 16 of 14.11.2016.
Results and Disscution
The results of determining the parameters of pure tone audiometry depending on the threshold value of hearing performed at frequencies of 125-12500 Hz for air conduction are shown in Table No. 1. It was found that at all degrees of deafness there is a change in the hearing threshold at frequencies in the entire range studied. A statistically significant veracity of the results of pure tone audiometry in accordance with the degree of deafness is highlighted (P<0.001).
 Table 1. Distribution of patients in the base group by degree of deafness (PTA)
Table 1. Distribution of patients in the base group by degree of deafness (PTA)
SA was performed on 18 people from the control group and 70 patients from the base group (Table 2). In the control group, AV indices characteristic of normal hearing were recorded (detection threshold 10.44 dB; vocal recognition threshold – 30.44 dB; maximum recognition score – 44.56 dB). In patients with deafness, 2 types of curves were determined. In most patients, upon reaching a certain threshold of clarification (80%, 100%, sometimes even a lower level), the subsequent increase in sound intensity leads to a paradoxical decrease in speech intelligibility. Another type of SA is characterized by a “steep” increase. The level of intelligibility reaches 100%, but the range of clarification is reduced, with increasing intensity of vocal sounds the intelligibility threshold decreases. The maximum recognition score for severe and profound deafness was not recorded in any case (Figure 1).
Figure 1: Speech Audiometry Curve
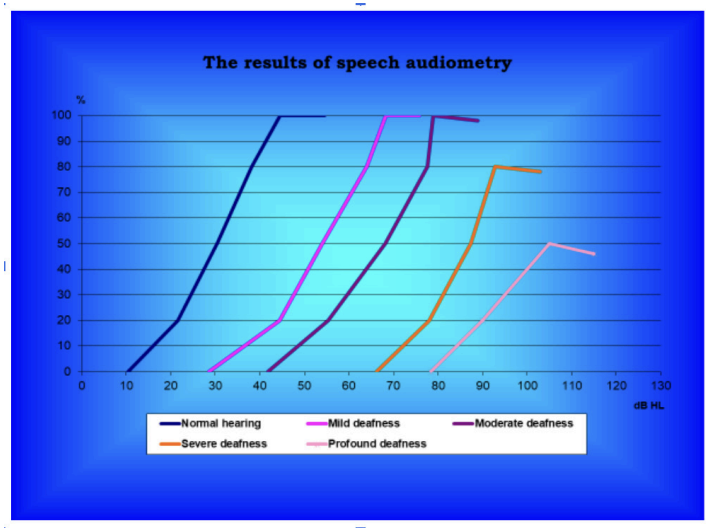
A statistically significant correlation is found between the degree of hearing loss and all components of SA: simultaneously with the increase in deafness, the percentage of intelligibility decreases. SA has an undeniable importance in subjective testing of the auditory analyzer [18].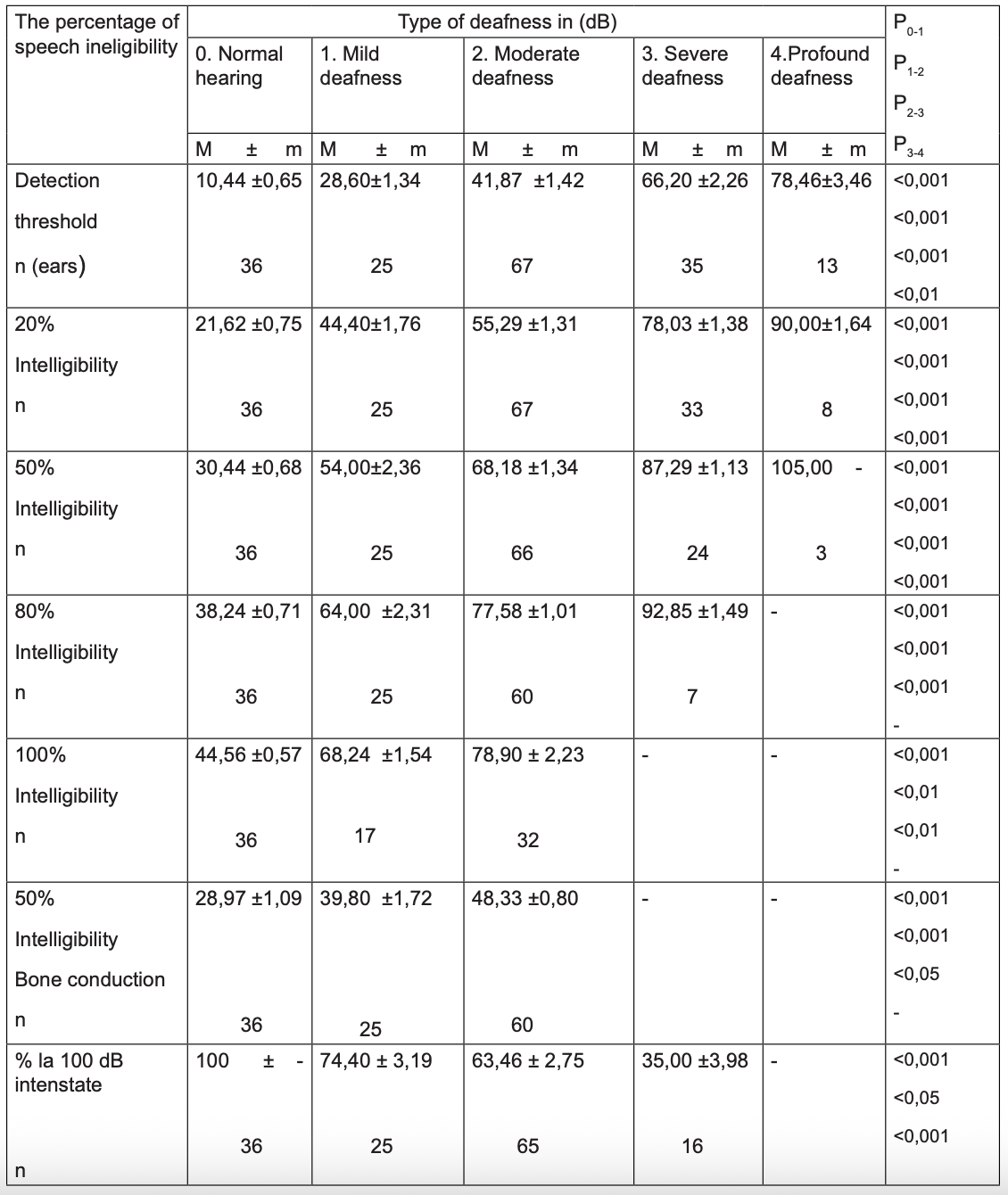
Table 2: Speech Audiometry Results
Notă: n – the number of ears for which the percentage of intelligibility was determined
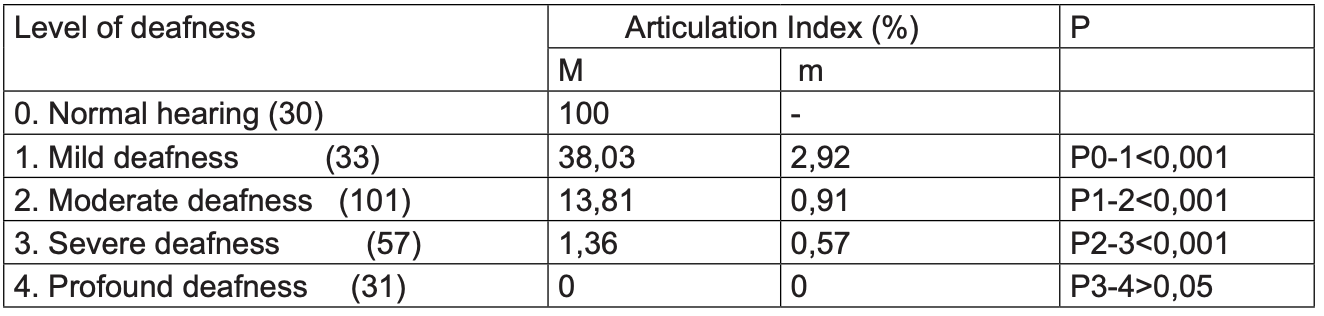
Table 3: Articulation Index calculated based on PTA results
According to the data of tonal audiometry, the articulation index of A. Pavlovič [7, 16] was established. A statistical correlation was established between the mild-moderate and moderate-severe forms of deafness and the IA data (Table 3). With a low articulation index, the effectiveness of hearing aids also becomes low. Based on the IA values, it can be stated that with different forms of deafness, the auditory verbal capacity changes and decreases retroafferently in proportion to the degree of deafness.
The essence of the proposed method consists in selecting the criteria for determining the maximal speech intelligibility score (MSII) based on the results of pure tone audiometry (when we can not do the speech audiometry) according to the formula, which includes the following parameters [8].
MSII= 0,784 x AH + 0.23 x DT - 1,192 x AC - 0,214 x IA - 0,59 x LD + 51,055 (constant index dB)
Where:
AC - aspect of the audiometric curve determined at the threshold audiometry descending – 1, steep descending – 2, flat – 3, ascending – 4 bell-shaped – 5;
AH - average hearing threshold established at the PTA; (100-6000 Hz), measured in dB;
LD - average degree of deafness established at the PTA; (500, 1000,2000 Hz) measured in dB;
DT- average discomfort threshold established at the PTA (500-4000 Hz), measured in dB;
IA articulation index, established on the basis of threshold audiometry (%).
A maximum speech intelligibility score recorded up to and including 40 dB is characteristic of normal hearing. A maximum score recorded at values higher than 40 dB is characteristic of hearing loss. The difference between the predicted maximum intelligibility score and the real one (the difference between the real and the predicted value) determined within the limits between 0-5% - being considered excellent; >5 -10% good; 10% - low.
The control of the proposed model on real data allowed us to find that an error that does not exceed 5% of the real value constitutes 54.9%, and an error that does not exceed 10% of the real value – 94.1% of the number of ears investigated.
The coefficient of determination (R2) for the model in question, in the tested patients, being quite high: R2 = 0.7255.
The coefficient of determination R2 with values between 0-0.2999 being unsatisfactory; 0.3000-0.6999 satisfactory; 0.7000- 1 high.
The result is an increase in the effectiveness of audiometric diagnostics by a more effective, operative and inexpensive method.
Example of use: Patient N., 37 years old, diagnosed with moderate bilateral sensorineural deafness. Pure tone audiometry was performed within 15 minutes, vocal audiometry was performed within 25 minutes. The analysis of the liminal and supraliminal pure tone audiometry performed automatically established the following indices: the aspect of the AC – descending; the average hearing threshold (AH) established by PTA – 45 dB; the level of deafness (LD) established by PTA – 48 dB; the average discomfort threshold (DT) – 101.25 dB, the articulation index (IA) – 23%. The maximum intelligibility score established within the 100% speech audiometry was set at the intensity of 75 dB, characteristic of hearing loss.
`When using the developed mathematical formula for predicting the maximum intelligibility score, we obtained the value 75.19 dB, the difference between the actual and predicted value being 0.25%, which represents a favorable indication.
Analysis allowed to calculate that an error not exceeding 5% of the real value constitutes 54.9%, and an error not exceeding 10% of the real value – 94.1% of the number of ears investigated. An indication for the use of this method is the audiological diagnosis of patients with deafness for the purpose of subsequent preparation of the treatment protocol and electroacoustic rehabilitation of hearing.
The advantage of the developed method is the objectification of the maximum speech intelligibility score. The developed method allows diagnosis in the absence of specific voice audiometry tests, does not require additional equipment, takes less time, which is subsequently important in the faster initiation of the treatment and rehabilitation program for people with hearing disabilities. The method facilitates the diagnosis of auditory pathologies and the individual prosthetic recovery program.
The indication for using this method is the audiological diagnosis in patients with deafness for the purpose of the subsequent preparation of the drug treatment protocol and electroacoustic hearing rehabilitation. There are no contraindications. The proposed method for predicting the maximum speech intelligibility score, which includes the analysis of PTA investigations allows for the establishment of an adequate diagnosis in the absence of specific voice audiometry tests and equipment, and can be used if the audiological office is not equipped with such equipment.
Conclusions
Was obtained increase the effectiveness of audiological diagnosis, thanks to a method for predicting the maximum speech intelligibility score.
The advantage is in objectifying the prediction of the maximum speech intelligibility score. The proposed method allows establishing the diagnosis in the absence of speech audiometry tests, which is subsequently important in the rehabilitation and, as a result, in the integration into society of people with hearing disabilities.
Audiometry examination is performed by setting the following parameters: appearance audiometric curve, the average hearing threshold, degree (level) of deafness, the average threshold of discomfort, articular index, then the results are used to calculate the speech intelligibility score.
References
- Shannon R, Basket D. Speech recohnition under conditions of frequency place compression and expansion. In: Journal Acoustic. Soc. America. 2003 Apr. Vol. 111 (4 Pt 1). P. 2064-2076.
- Cherko M, Hickson L, Bhutta M. Auditory deprivation and health in the elderly. In: Maturitas. 2016;88: pp. 52-57.
- Parii S. et al. (2025). Preclinical Research Optimization of Medicinal Products with Action of the Inner Ear. J Medical Case Repo 7(4):1-4.
- Stachler RJ, Chandrasekhar SS, Archer SM et al. Clinical practice guideline: sudden hearing loss. Otolaryngol Head Neck Surg. 2012 Mar;146(3 Suppl):S1-35.
- Lalain M, Ghio A, Giusti L, Robert D, Fredouille C, Woisard V. Design and development of a speech intelligibility test based on pseudowords in French: Why and how? J Speech Lang Hear Res. 2020;63(7):2070-83.
- Parii S. Improvement of diagnosis and pharmacotherapy of the ear disorders. Annotation of PhD Thesis in Medical Sciences.
- Pavlovic Ch. The speech intelligibility index standard and its relationship to the articulation index, and the speech transmission index. J Acoust Soc Am. 2006;119(5):3326.
- Parii S, Jucovschi C. Method for the determination of Speech Intelligibility Score. Patent no MD 792 Z 2014.09.30.
- Joint Committee on Infant Hearing (2007) Year 2007 Position Statement: Principles and Guidelines for Early Hearing Detection and Intervention Programs. In: Pediatrics 120, pp.898-921 doi:10.1542/peds.2007-2333.
- National Institute on Deafness and other Communication Disorders (NIDCD). Statistics and epidemiology.2025.
- Zhang Y., Jiang Q., Wu X. et al. The Influence of Metabolic Syndrome on the Prognosis of Idiopathic Sudden Sensorineural Hearing Loss. In: Otol Neurotol. 2019, vol.40(8), pp. 994-997.
- Wilson BS, Tucci DL., Merson MH., O’Donoghue GM. Global hearing health care: new findings and perspectives. In: Lancet. 2017, vol. 390 (10111), pp. 2503-2515.
- Stiles DJ, Bentler RA, McGregor KK. The speech intelligibility index and the pure-tone average as predictors of lexical ability in children fit with hearing aids. J Speech Lang Hear Res. 2012;55(3):764-78.
- Taghavi SMR, Mohammadkhani G, Jalilvand H. Speech Intelligibility Index: A Literature Review. Aud Vestib Res. 2022;31(3):148-57.
- Leal C, Marriage J, Vickers D. Evaluating recommended audiometric changes to candidacy using the speech intelligibility index. Cochlear Implants Int. 2016;17(Suppl 1):8-12.
- Sherbecoe RL, Studebaker GA. Audibility-index predictions of normal-hearing and hearing-impaired listeners’ performance on the connected speech test. Ear Hear. 2003;24(1):71-88.
- Canete, O.M.; Marfull, D.; Torrente, M.C.; Purdy, S.C. The Spanish 12-item version of the Speech, Spatial and Qualities of Hearing scale (Sp-SSQ12): Adaptation, reliability, and discriminant validity for people with and without hearing loss. Disabil. Rehabil. 2022, 44, 1419–1426.
- Radulescu, L.; Astefanei, O.; Serban, R.; Cozma, S.; Butnaru, C.; Martu, C. The Validation of the Speech, Spatial and Qualities of Hearing Scale SSQ12 for Native Romanian Speakers with and without Hearing Impairment. J. Pers. Med. 2024, 14, 90.
Disclaimer / Publisher’s Note:
The statements, opinions, and data presented in all publications are solely those of the individual author(s) and contributor(s) and do not necessarily reflect the views of YellowMark Publishing House, the journal, or the editor(s). The publisher and editor(s) disclaim any responsibility for any injury to persons or property resulting from any ideas, methods, instructions, products, or procedures referred to in the content.
©2026 Author(s). Published by YellowMark
This article is distributed under the Creative Commons Attribution License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.